Harm Reduction Guide
How to stay safe with psilocybin — dosage, set and setting, what to do if things go wrong, and who should not use psilocybin.
Harm Reduction and Psilocybin
Harm reduction is a public health approach: it gives people practical ways to reduce risk without pretending risk can be erased. For psilocybin, that means screening for medical and psychiatric red flags, avoiding dangerous drug combinations, using a safer setting, arranging sober support, and knowing when peer support is enough versus when emergency care is needed.
This page is educational, not medical advice. Psilocybin remains illegal in many places, and even legal or supervised settings require careful screening. If you take prescribed medications or have a mental health diagnosis, talk with a qualified clinician before making decisions.

Quick Safety Summary
- Do not use psilocybin during an acute mental health crisis, when you may harm yourself or others, or when you cannot keep the environment physically safe.
- Do not combine psilocybin with lithium or MAOIs. These are high-risk combinations.
- Do not abruptly stop SSRIs, SNRIs, mood stabilizers, or antipsychotics to make psilocybin "work better."
- Have a trusted sober sitter for first experiences, higher doses, trauma material, or any setting where judgment and coordination matter.
- Avoid alcohol, cannabis, stimulants, and other psychedelics on session day.
- Call emergency services for seizure, loss of consciousness, chest pain, severe breathing trouble, active self-harm risk, or an unsafe environment.
Before Anything Else: Screen for Stop Signs
Pause and seek medical or psychiatric input before any session if any of these apply:
- Personal history of psychosis, schizophrenia, schizoaffective disorder, or a recent manic episode.
- First-degree family history of schizophrenia or psychosis.
- Bipolar I disorder or unstable bipolar-spectrum symptoms.
- Current lithium use, MAOI use, tramadol use, or a complex medication list.
- Uncontrolled hypertension, significant cardiac disease, history of stroke, or active seizure disorder.
- Pregnancy or breastfeeding.
- Current suicidal ideation with plan or intent.
Screening is not gatekeeping. It is the part of the process that prevents avoidable harm.
Know What You Are Taking
The first rule is still simple: know the substance. Licensed programs use controlled products. Outside licensed settings, uncertainty rises quickly.
- Dried mushrooms can still be misidentified, especially by beginners or with wild specimens.
- Gummies, chocolates, pressed pills, powders, and "mushroom blends" may contain no psilocybin or may contain other psychoactive compounds.
- Reagent testing can reduce uncertainty but cannot prove exact dose, rule out every adulterant, or make an unsafe setting safe.
- If a mushroom was wild-picked and there is any chance of amatoxin-containing lookalikes, treat that as a poison-control issue, not a trip-support issue.
Dose Conservatively
Psilocybin potency varies by species, batch, storage, preparation method, and individual sensitivity. No internet chart can predict your response.
Use conservative principles:
- Start lower than your ambition. You can choose another session later; you cannot untake a dose.
- Avoid redosing during the peak. It can extend confusion without adding clarity.
- High-potency varieties and extracts can make weight-based advice misleading.
- Lemon tek, tea, fasting, and cannabis can change onset or intensity.
- Plan for at least 6 to 8 hours with no driving, childcare, work obligations, or public responsibilities.
Set, Setting, and Sitter
Set is your inner state. Setting is the place and people around you. A sitter is a sober person who can help keep the environment safe.
A safer session has:
- A private, familiar space with no surprise visitors.
- Water, bathroom access, blankets, gentle lighting, and a place to lie down.
- Phones silenced except for emergency access.
- No driving, cooking over flame, swimming, climbing, or wandering into public spaces.
- A sober sitter who knows the dose, expected duration, emergency contacts, and when to call for help.
A sitter does not need to interpret the experience. Their job is calm presence, safety, and escalation if needed.
Difficult Experience or Crisis?
Many difficult experiences are intense but self-limiting: fear, crying, confusion, grief, shame, body sensations, or reliving painful memories. These can sometimes become meaningful when the person is safe and supported.
Escalate beyond ordinary support if there is:
- Seizure, loss of consciousness, or inability to be roused.
- Chest pain, severe breathing trouble, signs of stroke, or extreme cardiovascular distress.
- Active self-harm, violence risk, or an environment you cannot make safe.
- Psychosis-like symptoms, mania, or severe agitation that continues after drug effects should be resolving.
- Possible poisoning from unknown wild mushrooms.
For non-emergency psychedelic distress, Fireside Project lists phone/text peer support at 623-473-7433 and describes it as support during and after psychedelic experiences. For medical emergencies, call emergency services.
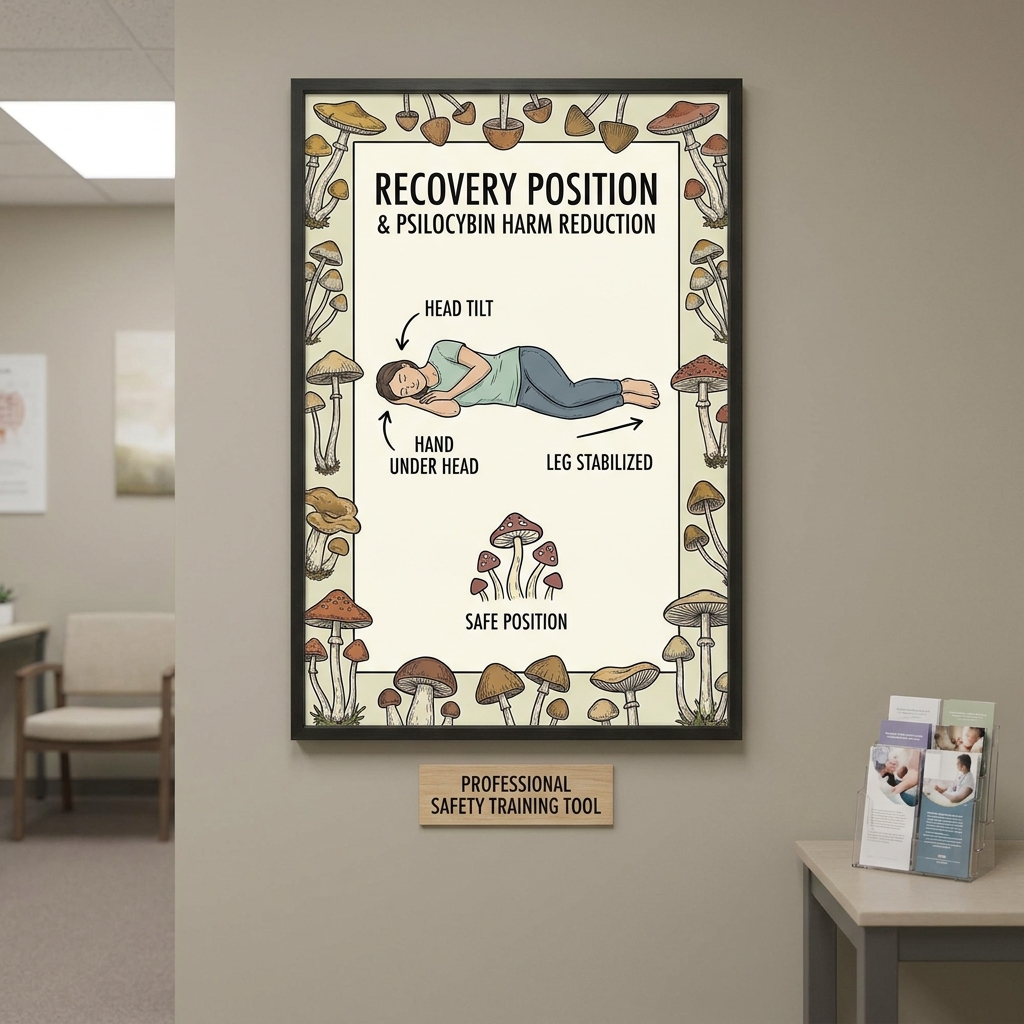
Supporting Someone Through Difficulty
Use low-force support first:
- Speak slowly and simply: "You took psilocybin. You are safe. I am here. This will change."
- Reduce stimulation: lower lights, soften or stop music, reduce crowding.
- Offer water, a blanket, a different posture, or a quieter room.
- Invite grounding: feet on the floor, one slow breath together, naming the room.
- Do not argue with visions, shame the person, or demand that they explain the experience.
- Do not restrain unless there is immediate physical danger.
Zendo Project frames psychedelic care around safe space, sitting rather than guiding, talking through rather than down, and treating difficult experiences as potentially meaningful when the person is safe.
Medication and Substance Cautions
The shortest practical version:
- Lithium: do not combine; seizure reports make this one of the clearest red flags.
- MAOIs: do not combine outside specialist supervision; effects may be intensified and prolonged.
- SSRIs/SNRIs: effects may be reduced, but stopping suddenly can be dangerous.
- Tramadol and serotonergic drugs: require medical review because serotonin toxicity is a concern.
- Antipsychotics and benzodiazepines: may reduce or block effects; do not change use without prescriber guidance.
- Cannabis: often intensifies confusion, anxiety, and paranoia.
- Alcohol and stimulants: increase avoidable risk and interfere with the session container.
See Drug Interactions for the fuller medication guide.
After the Experience
The first 24 to 72 hours matter.
- Rest, eat gently, hydrate, and keep obligations light.
- Avoid major life decisions while emotions are unusually open.
- Write down what happened before memory reorganizes it.
- Talk with a therapist, integration provider, trusted friend, or peer-support line if the experience remains troubling.
- Seek professional help if distress persists, sleep collapses, mania appears, suicidal thoughts intensify, or reality testing does not return.
Source Links
- Fireside Project Psychedelic Support Line
- Zendo Project harm-reduction principles
- Drug-drug interactions involving classic psychedelics: systematic review
- Acute adverse effects of therapeutic doses of psilocybin: systematic review and meta-analysis